Dr. Damian Dupuy, MD, FACR speaks about high-power RFA (HP-RFA) for a variety of tumor types using the Cambridge CRF system. He contrasts HP-RFA with microwave ablation (MWA), cryoablation (cryo), and lower-power RFA systems based on his 35-year pioneering experience in tumor ablation. This talk contains numerous clinical pearls for optimizing technical success, minimizing procedure time and complications, and selecting generator and probe parameters.
Dr. Dupuy is an Adjunct Professor of Diagnostic Imaging at Brown University and the Director of Tumor Ablation at Cape Cod Hospital. He has more than 3 decades of clinical experience and has authored over 200 clinical articles in the field of tumor ablation. This lecture was delivered at the Annual Scientific Meeting of Society of Interventional Oncology (SIO) on February 6, 2026.
Key Points
- High-Power RFA (HP-RFA) provides for efficient ablation of a wide variety of tumor types and sizes.
- HP-RFA has advantages over MWA, Cryoablation, and older, lower-power RFA in terms of speed, control, versatility, ergonomics, and pricing.
- RF electrodes have low imaging artifact and measure tip temperature, providing an objective basis to adjust the ablation zone intraoperatively to help prevent over- and under-treatment.
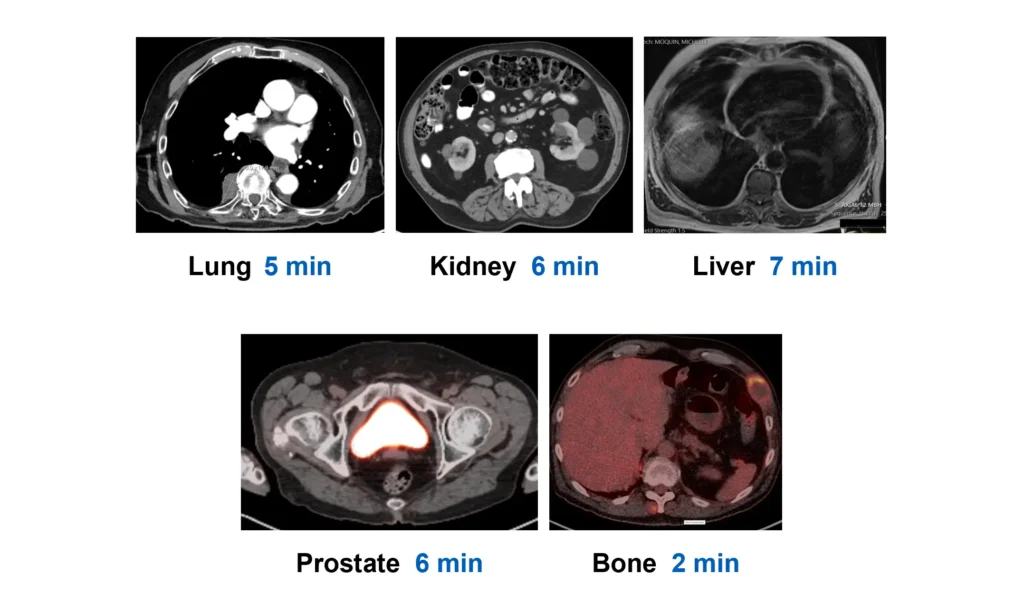
RFA Cases Presented
- Lung: Melanoma metastasis, 5-minute RFA
- Kidney: RCC, 6-minute RFA
- Prostate: Metastatic Prostate Adenocarcinoma, 6-minute RFA
- Liver: Dome HCC, 7-minute RFA
- Bone: Metastasis from lung cancer, 2-minute RFA, palliative
Transcript
Introduction & RFA History
My name is Damian Dupuy. I’m an interventional radiologist, or interventional oncologist, and I’ve been doing RF ablation since 1991. How many of you were born after 1991? 1… 2… 3. Okay. You probably haven’t heard the term “radiofrequency”. Well, radiofrequency has been around a long time.
Bernard Cosman developed the first RFA device in 1950 for nerve ablation, and that is the grandfather of the inventor of high power RFA. The grandfather.
Now, who was the father and what did the father develop? Does anybody know? The Cool-tip. The Cosman Coagulator was developed by the father and that’s Eric R Cosman.
Now, the son or the grandson is the developer of Cambridge Interventional, and that’s Eric R. Cosman Jr. He developed this high power RFA, and Nahum Goldberg who spent 25 years doing RFA science developed the algorithms of heating for this.
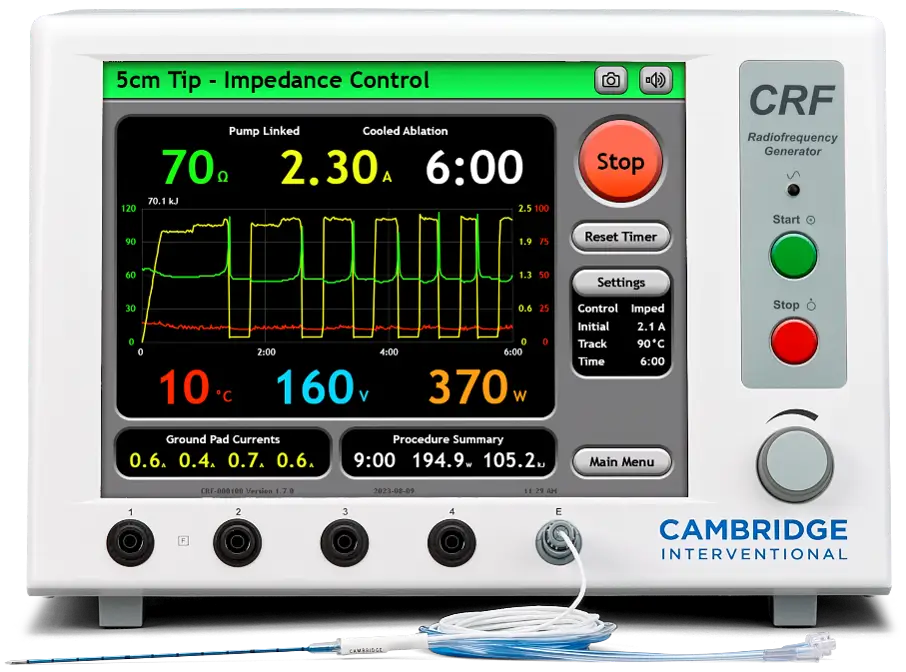
Cambridge High-Power RFA
This is the most highly sophisticated delivery device for RFA in the world. And, what I love about it is it gives you feedback continuously about the power that’s being delivered, the impedance.
It has multiple modes. You can do manual mode, and you can do pulsing mode. Pulsing mode is probably the best because it basically pulses and then when the impedance gets 20 ohms above the baseline then it shuts off again and it continuously does the pulsing and what it does is it keeps pushing power into the tissue.
The weaker RF electrode systems kind of fell by the wayside because they were replaced by microwave. Well, back to the future. Cambridge Interventional has so many more benefits than microwave. The algorithms and the user interface are much more sophisticated. Most of the microwave systems you see are kind of dumb, right? You push the button on, and it goes for 10 minutes. You have no idea what the tip temperature is because it doesn’t measure it at the tip. It can’t because that’s a patent infringement on Ted Ormsby’s device from San Diego. He’s had a 915 underpowered device which many people don’t even know exists. That’s very, very important.
370 watts is what this system can create. The last system that nobody uses anymore [could only produce 200 watts]. In fact, Medtronic bought it when they took over Covidien, and they don’t even use it, yet it’s more powerful than Osteocool, which is only 25 watts. So, you went from a 200 watt that’s in the closet somewhere, and you have Osteocool which is 25 watts. This is 370 watts.
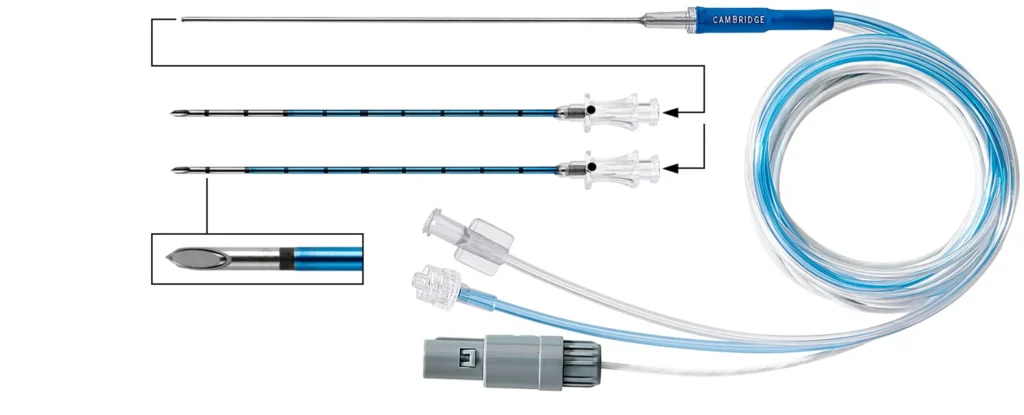
Cambridge RFA Electrodes
Look at the electrodes. They’re light. Look at the power cord. Super light. Long. There’s no loss of power with RF electrodes like there is with microwave, for which you have to have these bulky systems with bulky cooling. Super ergonomic.

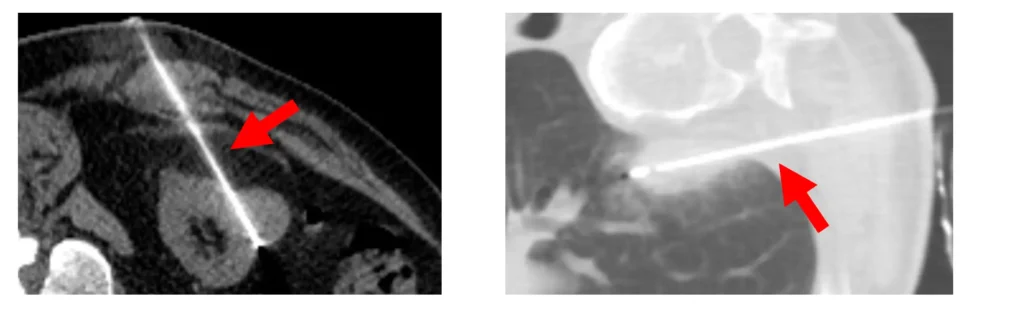
You know what? You will die when you look at these under CT fluoroscopy. No artifact. We all have seen the artifact of some of these bulkier microwave systems. That’s because it’s high atomic weight metal. The more metal, the more artifact. This is the least artifact applicator in the world for RFA or microwave.
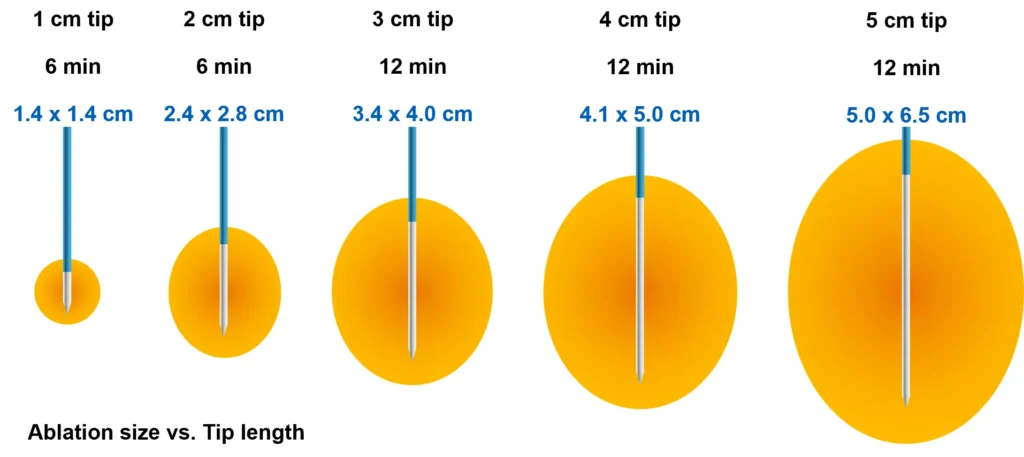
These are the various types of electrodes that Cambridge Interventional makes, and they’re pretty cool actually. Above the 1 cm tip– obviously, the 1 cm is used for thyroid– they make a 2 cm tip, a 3 cm tip, a 4cm tip in 17 gauge, and a 5 cm tip in 15G. Amazing array of what you need to use when you’re an interventional oncologist.
Coaxial RFA Electrodes – Biopsy & Drug Delivery
My favorite is this one. This one is a cannula. You can place it into the patient directly, do a biopsy, do whatever through the stylet, and then this activates it as an RF electrode. Think about the applications you could do with that. I’m just going to pass it on. That’s really cool. You can deliver drugs. Obviously, you’ve heard the lectures this week about direct drug delivery. Well, you can deliver the drug, you can do your ablation, and then let the immune effects of the drug take place.
Electrode Temperature – Ablation Confirmation & Sculpting
The thermocouple is key though. I use the thermocouple in every single case. When you’re perfusing the electrode with the cooled water, you want to know exactly what’s happening at the tip of the electrode. That’s the business end. You shut off the pump, and then you watch the thermocouple rise and the temperature rise. We know 60 °C is immediate cell death. You will often see this 70-80 °C at the tip. You then while you have this hot zone can move this very delicate needle and place it somewhere else. You can see it with CT fluoro. You know exactly where it is. It’s precision medicine at its best. You can sculpt the lesion. You can overlap your ablation. You can say, “I don’t need to do another treatment there. It’s telling me it’s 80 °C at a centimeter away from where I just was.” You’re using that constant feedback. We do not have that with microwave. Microwave, you either underheat or you overheat. You’re rarely perfect.
RF vs Microwave Probe Cost
Let’s talk about the cost. [An RF electrode costs about $1,000.] How many people here know what a microwave antenna costs? How much does it cost? $2,500. He says $2,500. Anybody Any other takers? Anybody from the industry? How much does your antenna cost? $2,200. $2,200. Okay. Well, I know there’s one that charges over $3,000. That’s disposable. So, if you use two, you lose money on every single case.
Lung Case – Melanoma Metastasis
Let’s talk about some cases. Here we have a patient with a solitary pulmonary nodule in the right lower lobe kind of right next to the pleura. People always talk about, “I can’t treat near the pleura. I’ve got to use cold.” Okay, I’ve been treating against the pleura [with heat] for my whole career. How do you do it?
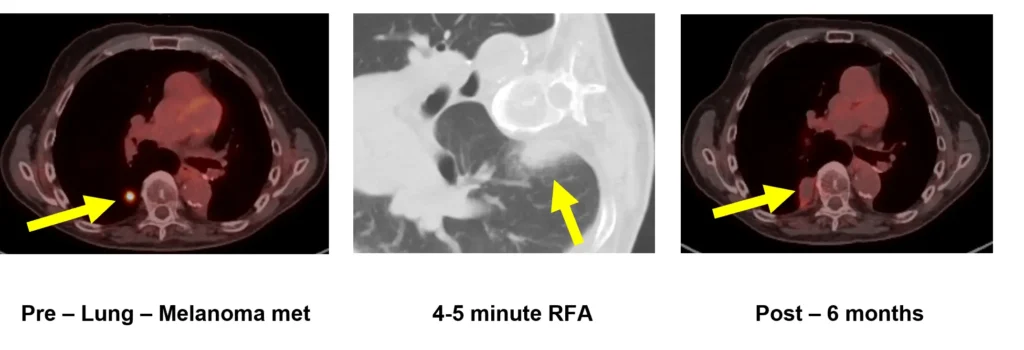
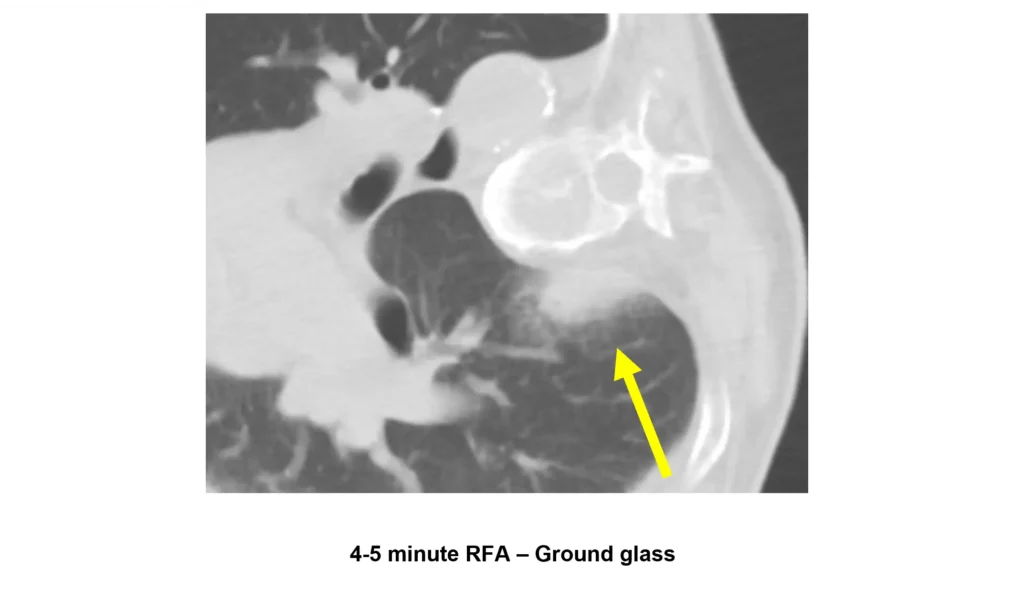
Well, in this particular case, patient is on his side. I’m coming in posteriorly. I use a 22 gauge needle and I place it in the paraspinal soft tissues and I put in first of all 1% buffered lidocaine and then I put in 30 ml of bupivacaine. I create this huge area of no muscle activity at all in that part of the rib cage which helps in reducing pneumothorax. I’m pushing the tumor closer to the central lung so I’m further away from the intercostal nerves, so I have less chance of in damaging them. I’ve done that in this case and then I turn on the power and I treated this patient for about 4 minutes and you can see after the treatment we have this beautiful ground glass halo which indicates leakage of fluid into the capillary bed. that’s been damaged. To me, I’m very happy. This took less than five minutes. Because of all that fluid I placed there, the patient had no symptoms. I use light sedation. I start off with intravenous lorazepam, and I might give them half doses of versed and fentanyl, 25 mics and 0.5.
Here is the patient’s follow-up. This is a six-month FDG PET and we can see the thermal scar. Uh we can actually see the needle tract. Notice there’s no plural effusion. It’s a great, great treatment. Why would you want to do cryo here? Do you think you could do a better job with cryo? Do you think you could do cryo in four minutes?
RFA vs Cryo – Number of Probes & Cost
What is the cost of cryo? How many probes do you have to use? At least two, right? Well, if you have high-power RFA in your department, why wouldn’t you use it? Because you don’t know about it because you started your training when people had already abandoned the low-power RF. It’s sitting in a closet collecting dust somewhere. You should be using high-power RFA because it’s faster, it’s cheaper, it’s easier to use, no artifact, it’s just a no-brainer.
Kidney Case – RCC
All right, kidney and lung are my two most common ablation parts of the human body. Here we have a typical patient who gets scanned in the ER. They’ve got a bunch of cysts, but they also have this solid enhancing cyst that you can see on the lateral right kidney. It’s not as vascular as the kidney. Typically, renal cells aren’t as vascular as the kidney. You might get an aggressive renal cell that’s hypervascular, but most of them are less vascular than the kidney, so they’re very easy to ablate with RF. If you’re going to use cryo on this, I’m going to be on my third case with RF while you’re still finishing your first cryo case.
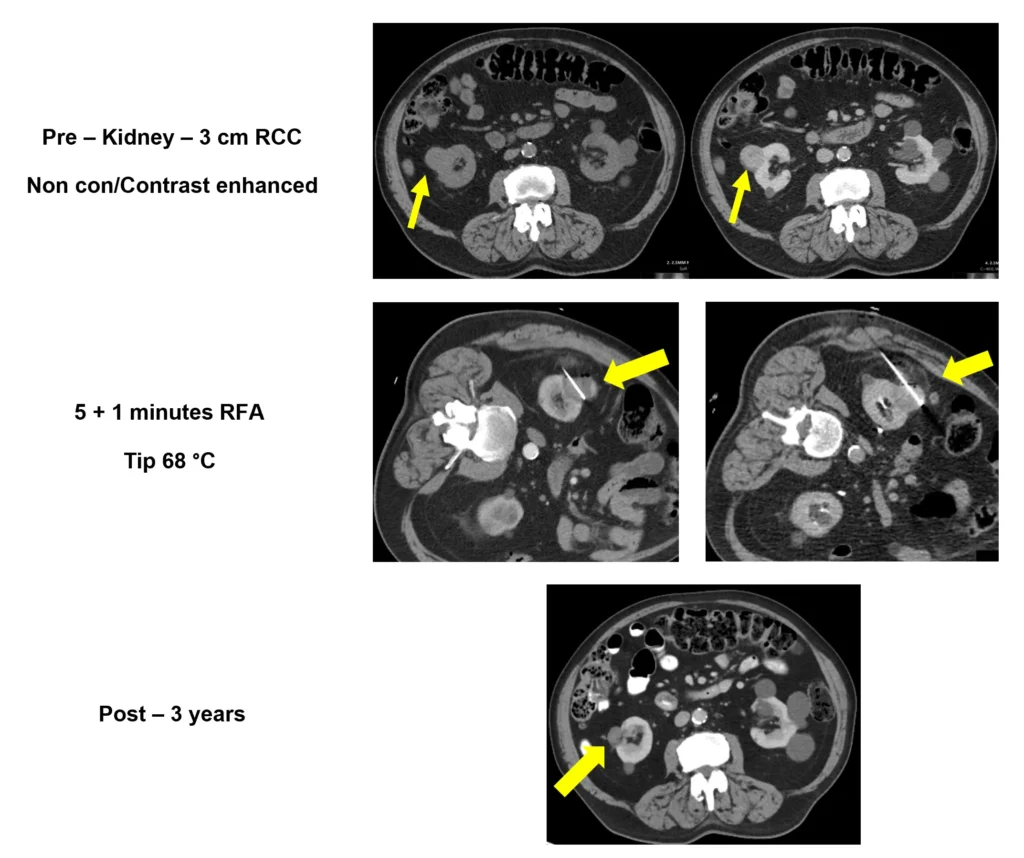
In this particular patient, I put them to decubitus, and I want to amputate the tumor from the cortex. I place [the electrode] right along the junction with the normal kidney. Look how easy it is to see the tip of the electrode. The tip is hyperdense because that’s where the cooling channels fuse, so you always know where you are. You get about 4 mm of heating beyond the tip, but there’s a lot of fat there. That energy isn’t going to go anywhere. We treated this patient. What I always do is I look at the parameters and I say, “Okay, I think I cooked it completely. We had quite a few high temperature spikes. This was a five minute ablation and I do the contrast study with the needle still in because it has no artifact. I can do that, and I can see the ablation zone. See the ablation zone on the cortical side? That’s a great margin. But, there was probably a little feeder maybe on the outside. So, what do I do? Well, there’s some residual enhancing tumor. Well, it’s very simple. I pull it back a couple centimeters. I angle it and I pop it back in and I do another ablation. 1 minute and you can see the changes on the lateral in the fat. 1 minute and I got to 68 °C. So, I’m done. I’m done. I’ve coagulated the tract, right? So, I don’t have to worry about bleeding. I pull the needle out. I’m done. I tell the patient, “I’ll see you in 6 months.” That’s what I do. I do a verification CT. If it’s completely dead, I see you in 6 months. Why do I need to see you sooner? Unless you have symptoms, it’s a waste of time. These things are slowly growing. If this is dead, it’s going to be pretty much dead in six months and dead forever. Here’s a 3-year post. Unlike cryo though, with RF, you’re coagulating protein, so you denature it. The body walls it off. It’s a foreign body reaction. You may see some contraction over time, but most people will have a scar in their kidney for their entire lives. As long as it’s not enhancing and it’s not growing, it’s not hurting anybody.
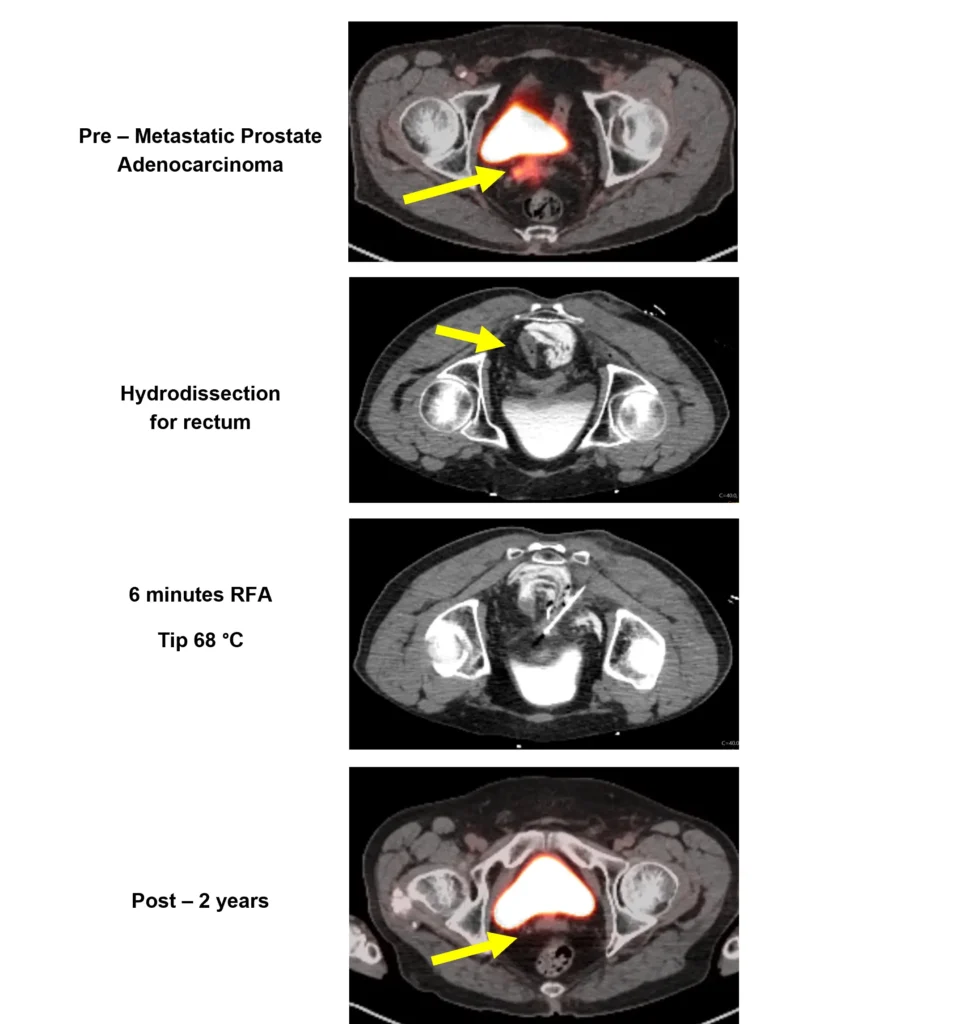
Prostate Case – Metastatic Prostate Adenocarcinoma
Here’s an interesting case. I don’t know if any of you went to the prostate session earlier today. They were talking about treatment of recurrent cancer of the prostate gland. This is a gentleman who had a Gleason 7 with a PSA of 14.7 because he had bone mets and radiation therapy to the primary as well as to the pelvis, and his PSA was going up. You can see there is a soft tissue mass anterior to the rectum posterior to the bladder above the seminal vesicles. The radiation oncologist says, “Damian, can you treat this?” I say, “well it looks pretty good. I can probably hydrodissect the rectum if that’s a problem.”
We brought the patient in, made sure that he had an enema before he got on the table, and we can see the mass is very close to the bladder. In the image on the right, you can see the doped saline that I used actually didn’t use saline D5W to push the rectum to the opposite side and I was able to do a biopsy and put the electrode directly in the tumor. The biopsy came back metastatic prostate adenocarcinoma. I did 6 minutes of total heating with a T-max of 68 degrees and that was using impedance non-impedance mode. I used impedance mode for three spikes, and then I just kind of slowly titrated the energy down.
Here we have the one-year post PMSA and we can see that the lesion is completely cold, and here he is on two years. This is a great treatment for somebody who had really no other option. It was done with RFA and some hydrodissection.
Liver Case – Dome HCC
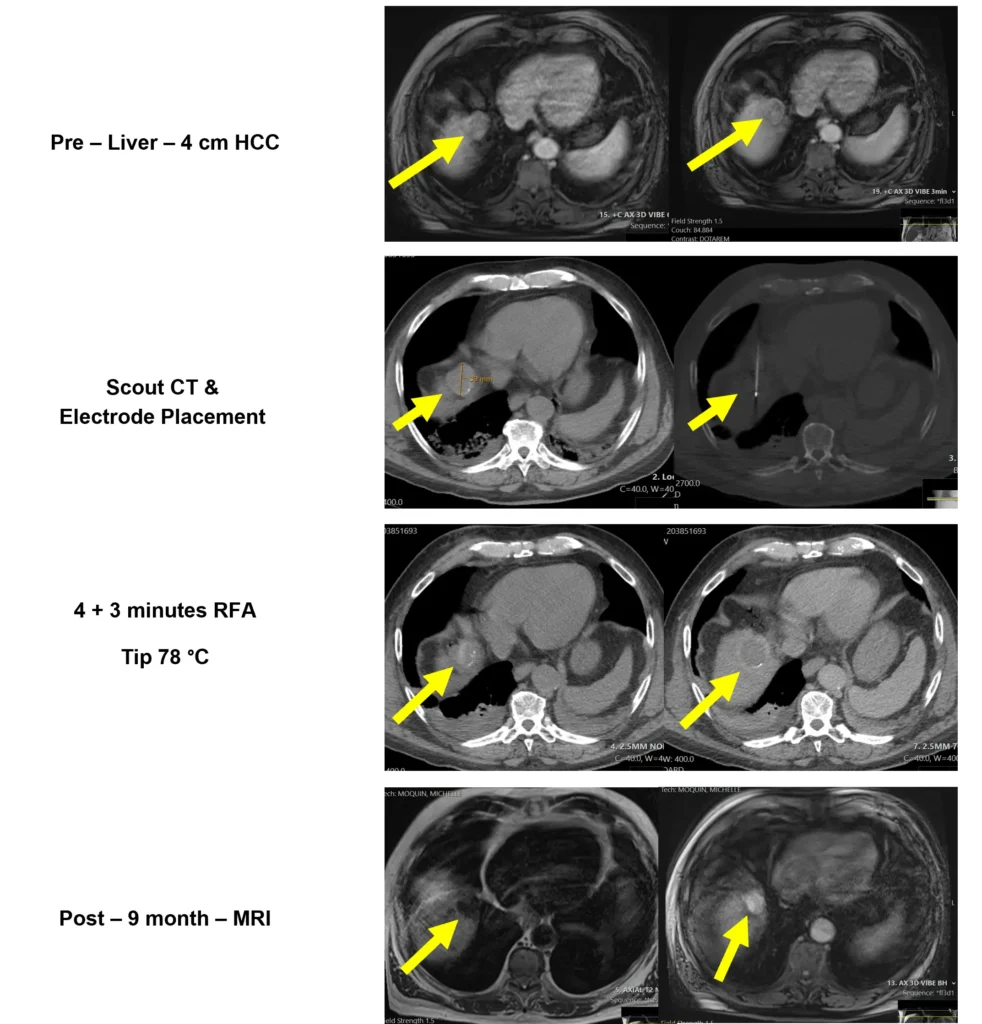
What about liver tumors? This is a case that came to me from the Beth Israel with a history of cirrhosis. They tried to do a biopsy and they missed the target and the patient was all upset. I looked at it and I said, “Well, why don’t we come from the anterior aspect and we can probably get our needle in there without having to worry about angling and, you know, potentially hitting the lung.” This is a lesion that had some arterial enhancement and you can see the wash out. It measured 4 cm.
Here we have the 3 cm active tip which was placed in the in the central portion of this tumor and we did a biopsy at the same time in the middle, and then you can see the tip of the electrode very nicely. It was a great location to treat anteriorly because it came right through the fat plane around the heart. We did a 4-minute treatment and a 3-minute treatment for a total of 7 minutes. This is a 4 cm HCC with a tip a maximum temperature of 78 °C. To me, that’s dead. He came back for a contrast and non-contrast CT scan. Actually, this was the day of the procedure. You can see the hyperdensity in the actual tract where the ablation was done. That’s because of coagulated protein, not necessarily hemorrhage. In the contrast study to the right, you can see the shell of the tumor.
Patient comes back for a follow-up MRI at 9 months. We can see the T2 dark, which is a typical post-ablation characteristic. T1 bright due to the blood products, and T1 shorting tissues and you can see that it doesn’t enhance on the arterial phase. It looks like it’s enhancing but that’s actually just the hemorrhagic products that you can see on the pre and if you do a subtraction you can show that there’s in fact no enhancement of the tumor. We were able to treat this tumor with a single needle with two placements in under 10 minutes. Certainly, you wouldn’t cryo this patient. If you microwave this patient, you probably would have had a lot more pain in the diaphragm because you probably overheated it because you can’t measure the temperature of the tip and you have no idea where the heat’s going.
High Power RFA Summary
In summary, Cambridge Interventional has low artifact electrodes. I think I’ve shown you that you’ve actually seen all the multiple sizes of the electrodes that are available. Certainly, everyone would agree that the ergonomics of this system is better than anything else out there. Why wouldn’t it be? You’ve seen it. It’s lightweight. It’s easy. The ablations are much faster because you don’t have to heat for an unspecified time because you can’t measure temperature and you don’t know what’s going on because you just push a button that said on. It gives you feedback. It’s a precision device. It’s a smarter ablation. And, it’s the most effective on the market. Thank you for your time. We’ll take some questions here.
Q&A – Electrode Temperature – Ablation Confirmation & Sculpting
Question for you. How do you assess that what is the total amount of energy you have deposited in the entirety of the tumor? Let’s suppose you’re treating a 2 cm nodule. You obviously know the temperature of the tip of the probe, but how do you assess that you have got adequate margins, and you know you have to read the entirety of the tumor, and how long does it take to get that?
Correct. The question was: how do you know what the temperature is away from the tip? The tip is your probe, so when you get to the maximum temperature in that spot, you pull back, and then you put it lateral, and then you measure the temperature. If the temperature is 80 °C, pull it back, measure it again, and you come out to the outer margin. If it’s 80 °C, you’ve killed it completely. In that particular case, I treated medially. I pulled out, and then I treated laterally. So, I did two ablations almost like a chopstick here and a chopstick there, but with one electrode.
Q&A – Selecting Electrode Tip Length
Question: If it’s a 2 cm tumor, would you use a 2 cm active tip?
You could do two, but you might want to pull back in tandem and do a second ablation on the proximal side or you could use a three. The benefit of the three is you use four grounding pads instead of two because there’s more metal and you can get more amps and you have 370 watts power. So, you can really blast these tumors but you’re not blasting them like microwave. Remember RFA doesn’t heat above you know 80-90 degrees Celsius. That’s how you’re interrogating what you’ve done.
Q&A – Ground Glass Margin in Lung
Question: In terms of tumor margin assessment, it’s just the ground glass halo that you assess?
Right, now Rob can explain that really well and I’m going to try to emulate him on this one. The ground glass is a mixture of live and dead tissue. The inner half is dead, the outer half is live. So, if you get a 2 centimeter margin of ground glass, you’re probably going to be perfect. When they do SBRT, they only want an 8 mm margin when they do their planning. So, you get a 1 cm on that. It turned out to be metastatic melanoma. That’s not coming back. I mean, that’s well cooked. The key [with RFA] is you only had to use one thin antenna, right? It’s a fraction of the cost of the disposal use if you had to cryo. And, the post-cryo irritation is so much more severe than it is by doing an ablation up against the pleura with an RF electrode.
Q&A – Type of Sedation
Question: All of the cases you should sedation?
They’re all done with sedation. I don’t use general anesthesia for lung cases. Never have. You don’t need it. You don’t need it. Bupivacaine is your friend. Lidocaine is your friend. Sedation is your friend. And I play music for my patients. I’m serious. It’s very healing and soothing.
Q&A – When do you not use RFA?
When do I not do RF ablation? If I have a large chest wall mass close to the skin, I’ll use cryo.
If I have a medially placed kidney tumor inferior that’s close to the ureter, I don’t like to do perfusion with heat and put in a catheter because that patient has to go to the O.R. for the C-arm to put that in before the case. What I will do is, I’ll have them put in a double J nephroureteral stent in their office or at another time and the patient will come back a week later and I’ll do the ablation with cryo with the stent in place and that protects the ureter and then they remove it two weeks later.
Cryo is great for certain things. RFA is greater for more things. Microwave has its moments. But, I would say that if I was starting out in a practice and my administrator said you can only buy one system, if you didn’t buy this system, you would be doing yourself a disservice.
Q&A – Historical Lung RFA Outcomes
Quick question. The data for local tumor control in the lung RF that came out during 2015 in Chest was a little bit on the lower side compared to microwave and cryo ablation that came out more recently. You think it’s because of the lower power RF systems in those cases?
Yes. All of us who cut our teeth on lung ablation with RF, we had an impedance problem, and you could never measure temperatures that were in the toxic range because it would shut off so quickly. You had no idea what you were doing. That’s why we did the triple electrode cool tip when I ran that NCI that trial multicenter trial because you could actually get more power in with the three times. But people were afraid of doing that because they’re like, “That’s three pokes. You’re going to have a more higher pneumothorax rate.” But with a single needle, you don’t need it now. It would be interesting if somebody wanted to do a trial comparing, you know, cryo and high power RFA. Do a three arm. You could do it with microwave, too. And I’m telling you, I haven’t put a chest tube in an entire year. I do probably I did 40 primary lungs last year, and I didn’t put a chest tube in.
Question: Do you use 16 gauge or 15?
17 gauge. Yeah. And what I do is in the extra plural space I inject lots of lidocaine and bupivacaine. It paralyzes the musculature for a good 12 hours. When you pull your device out, all that fluid under pressure kind of fills the hole. So, pneumothorax is a thing of the past. I quote my patients as about a 3% chance you’ll need a chest tube. Most people are saying 50/50. It’s like, you got to be kidding me. You know, learn a new technique, right?
Q&A – Bone RFA
Question: What about bone?
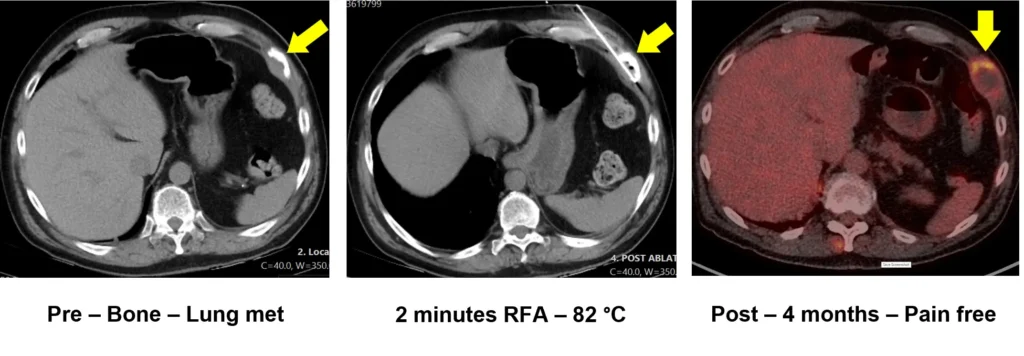
Bone. Yeah, bone is great. The problem with bone is if it’s not destroyed, you got to drill there, you know. But, I had a guy who had a tumor in his humerus, and I was able to drill and it was a long tumor and I was able to get an RF electrode all the way down the marrow space and heat it and pull back and treat it with a single RF electrode. That was kind of cool.
Question: Would you use it for palliative care?
That was palliative. Yeah, for sure. It works really well in bone. I actually ran a multicenter trial in bone for palliation and that was a positive study, and that was published before the cryo trials, you know, and people forget about that trial, but it works it works in bone.
[This transcript has been edited for clarity.]